A friend of mine – let’s call him Bobby – recently asked me for help on a bid he was writing which needed to include “innovative approaches”. Bobby expressed a clear dislike for the Developmentspeak term “innovation”. For Bobby, the term is just a fad.
So do I agree with Bobby?
The term “innovation” has become a popular buzzword in the development sector. There are plenty of examples, from USAID’s Development Innovation Ventures, to UNICEF’s Innovation Unit. The Guardian featured “12 days of innovations” over Christmas in 2013, profiling “eye-catching innovations in development”.
I do see some advantages to an emphasis on innovation. Calling for programmes to be more “innovative” encourages them to experiment more and try different solutions. This could generate unique ideas and new ways of approaching problems – just take a look at TechChange, Commcare, or FrontlineSMS.
However, many ‘innovations’ don’t actually contribute anything new, or do anything different. For example, I don’t see how telemedicine – using telecommunication and ICT to provide care at a distance – can today be seen as an innovation. Allowing patients to speak to health professionals over the phone came about in the UK in 1998 with NHS Direct!
Furthermore, there is a proliferation of pilots across the globe that are not being scaled up. A good example is mHealth, using mobile technology to help improve health. In 2008 and 2009 Uganda had 23 mHealth initiatives that did not scale up after they were piloted because the initial funding had dried up (see image below). It has reached the extent that some criticise the situation as a “pilotitis; a term used to describe a scenario where many NGOs are funded for relatively similar, but isolated, pilot projects, resulting in no resources left for scaling them up.
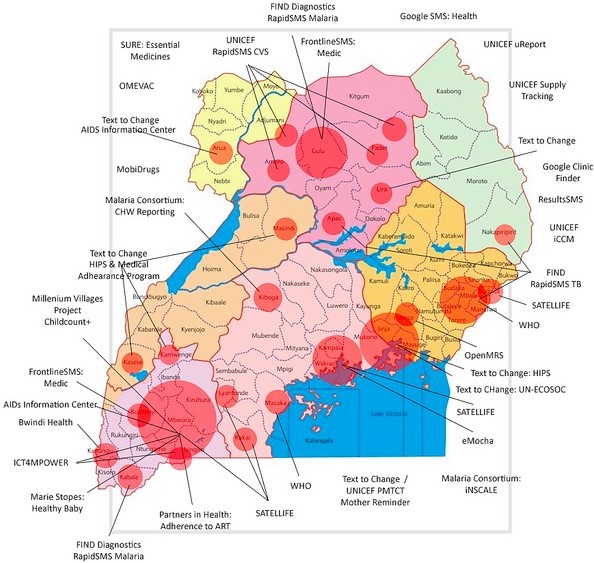
Map of Mhealth Pilots in Uganda. Source: Sean Blaschke, Technology for Development Specialist at UNICEF Uganda
The problem with “pilotitus” is that a lot of money is being wasted on these projects and the government has no idea what’s going on. In Uganda, it led to a moratorium on all mHealth projects being issued by the government.
What’s more, mHealth “innovations” have rarely been well monitored and rigorously evaluated. We need to ensure that monitoring and evaluation is taking place so that we know what’s going on and what works. This will (hopefully) mean that we can learn for future projects and reduce the risk of re-inventing the wheel.
So I ask myself again, do I agree with Bobby’s scepticism about innovation?
Encouraging innovations has led to great advancements and saved lives. I believe we should still encourage it, but always ensure that frameworks are in place to effectively monitor and evaluate these programmes’ progress. What do you think? Are innovations in the aid sector worth it?

Any industry needs to encourage innovation. Industries with as many failed or problematic practices, organisations and projects as the development industry could certainly use innovation – not just to create better projects, but to reshape the way actors go about tackling development.
That being said, I think your point that this can lead to a lot of wasted money if proper M&E isn’t put in place. I would also add that proper planning and an understanding of how long the ROI on innovation is likely to be also need to be given more credence.
One needs to be innately suspicious of efforts to put “moratoria” on innovation, especially in highly corrupt environments like Uganda. The moratorium is in fact a way to allow the Ugandan Ministry of Health to force donors to channel resources through it at a time when donors are beating a hasty retreat from direct funding (this after the prime minister’s office was implicated in several scandals involving donor money). Many promising investments by donors such as mTRAC which is implemented through the MOH have yet to prove their value after several years, which is why you won’t find any rigorous evaluations taking place anytime soon. Pilotitis is bad in a country like Rwanda with a clean efficient government, but i a country like Uganda, it at least offers a chance to donors to fund innovation that can then be handed over to civil society to implement, without getting entangled in corruption shenanigans.
Starting around 2011, at the cost of well over $5 million, UNICEF and the Ministry of Health of Uganda rolled out a text message system called mTRAC. From day one, it was launched with the nebulous claims that it was “changing lives”, “saving lives”, “reducing drug stock-outs”, “increasing accountability”, etc. mTRAC would fall very severely short of any serious positive impact. Looking back, it was laughable that anyone should have thought they could reduce the complexity of clinical care and supply chain management to more or less, random text messages. UNICEF and the Ministry of Health of Uganda have not published a critical review of its multi-million US Dollar splurge but neither has the duo continued to sing the praises of mTRAC.
On the device front, a smart phone app has been presented to none other than the President of the Republic of Uganda, His Excellency Yoweri Kaguta Museveni. The Matibabu Windows mobile app has won international acclaim at the Microsoft Windows competitions.
According to one of the developers, “….The Matibabu app uses red light to determine the state of the red blood cells to determine one’s malaria status.” That assertion is either truly ground-breaking technology worthy of The Nature magazine or it is outright pseudoscience.
Beyond any debate however, there are very basic tools known to modern science that can and must be used to assess the viability of eHealth innovations. These include Laboratory Efficacy Studies and Randomised Control Trials. Even before these methods, there is good old common sense to call upon. The Winsenga system, another celebrated Ugandan innovation, which consists of a Windows Smartphone attached to a microphone is designed to analyse and record the heart beat of a fetus and to save lives. It is not quite clear how the saving of lives is achieved by this app. Be that as it may, all Ugandan midwives are trained to use a plastic tube (that costs probably next to nothing) to listen to fetal hearts. There is no study to show that the Winsenga system is superior or even equal to the traditional, plastic fetoscope.
The developers who have innovated these products that may never be of any real value to the world of medicine are no doubt, brilliant. The software companies that encourage and reward them for using their platforms are doing what any reasonable corporation would do.
I am a medical doctor and technology evangelist. My call is by no means for a cessation of investment in health technologies, but rather for the ministries of Health and International NGO’s such as UNICEF and WHO to embrace time-honored practices that allow smart solutions to answer intelligent, medically insightful questions. The apparent, unscientific, free-for-all foray into the development of eHealth/mHealth innovations is wasteful and must stop.
This article potentially raises points of contention that I am more than eager to debate to a reasonable conclusion with the parties concerned.
Dr Edem Rukundo, FCS (ECSA)
edemrukundo@gmail.com
Pingback: Summer reading | kirstyevidence